Can artificial intelligence become your next personal trainer? One Maltese start-up is redefining fitness by merging AI, computer vision, and physiotherapy to create a virtual coach that understands your body’s every move – guiding you toward safer, smarter, and truly personalised exercise.
Imagine biting into a crisp apple, its flesh bursting with sweetness and tang. You might think of the vitamins, perhaps the fibre, or simply the refreshing taste. But hidden within its colourful skin and juicy flesh are hundreds of tiny compounds quietly working behind the scenes to protect your health. These invisible allies are called phytochemicals, and they are transforming how we think about food, nutrition, and sustainability.
Lara Sammut is finding answers to a long-standing challenge in the Obstetrics and Gynaecology Department at Mater Dei Hospital. Threatened miscarriage is a poorly understood condition that can lead to pregnancy loss, yet there is little data in Malta to help guide treatments and reassure families. Sammut’s research promises to change that.
Since 5G was announced, it has polarised public opinion. Many claim that it will revolutionise the world, while others fear that it poses a threat to our health. In Malta, the installation of new antennas on rooftops and public spaces has fueled debate. But what is 5G, how does it work, and is it actually dangerous? THINK speaks with Dr Julian Bonello, a researcher from UM’s Department of Physics, to separate fact from fiction.
For her second-year physiology research project conducted under the supervision of Chev. Prof. Renald Blundell from UM’s Department of Physiology and Biochemistry, Courtney Ekezie focused on sustainable food systems and their impact on human health. The study briefly mentioned culinary medicine – an aspect that later inspired this article for THINK.
In Malta, around 10% of the local population is affected by diabetes. This is especially alarming considering that diabetes can affect the blood and nervous system and eventually even lead to foot amputations. Researchers from the University of Malta (UM) and Mater Dei Hospital are trying to address this problem in their project Sit_Diab: Smart Insole Technology for the Diabetic Foot. They developed a novel method of detecting foot complications early enough to take action in time to help save limbs.
Parkinson’s disease (PD) is a complex, progressive, neurodegenerative condition affecting around 10 million people worldwide. But for every person directly struggling with PD, there is at least one carer, if not an entire family, dedicated to managing the disease. Are we doing enough to support these silent heroes? Cassi Camilleri asks.
‘I’m extremely anxious about her balance. Since the diagnosis, it’s been a constant nightmare because of the risk of falling and getting hurt. In reality, it’s only now that it’s started to become slightly affected,’ says Mildred Atanasio.
Mildred’s mother Rita was diagnosed with PD some years back after her husband passed away. One evening, Rita picked up one of her favourite novels for an evening read and noticed a tremor in her hand.
‘The worst part is when she tells me that all is ok and lovingly attempts to disguise a PD-caused stumble as something less worrying,’ Mildred continues.
‘She does this out of love, we know. She is worried about being a burden on me or my siblings, an idea which cannot be further from the truth. We all love her just the way she is. But this, coupled with my own fear and worry is rather draining… though I think sometimes my mind is worse than the actual symptoms.’
Though her experience is unique in many ways, the feeling of anxiety Mildred goes through is one she shares with many others.
The task of caring for another human being requires time and energy. According to the European Parliament Interest Group on Carers (EPIGC), carers spend an average of 22 hours per week providing for their loved ones. Even when this is done willingly and with love, without the right support network, it can leave carers susceptible to significant strains on their own physical, mental, and emotional health.
The same research by the EPIGC reveals that a third of carers lack sleep and feel depressed. Another third say that they are at a ‘breaking point’; one in five is unable to see anything positive in their life.
Close relatives often take on this important role; however, they often reject the term ‘carer’, seeing their work as a natural extension of the relationship with their affected loved one. ‘I am a daughter first. And the word ‘carer’ does not quite fit in my mental image of things,’ Mildred explains.
However, this has seen many go unrecognised for the service they provide for our community. Often, those who do not register themselves as carers are less likely and less able to access the services available to them.
You are not alone
Working hard to reverse this trend is the Malta Parkinson’s Disease Association (MPDA), with Veronica Clark at the helm as president.
MPDA informs citizens about PD and offers practical help on how to manage symptoms in the home. This includes talks by healthcare professionals so that people with PD and their carers are empowered to better manage their condition.
Peer support meetings foster a discussion about emotional and psychological needs and allow carers to cope with mental health issues they might be facing. Healthcare professionals are employed to further achieve this.
Mildred and her family make use and speak highly of these services. ‘Thanks to the MPDA, we have discovered and happily become part of a strong network of friends,’ Mildred says, a network she describes as very comforting. ‘We also share useful tips among us for day-to-day life which is nice.’
Giving a snapshot of the situation in Malta, Clark is quick to point out the benefits of our national healthcare system, which provides free treatment, accessible to people with Parkinsons in a whole range of disciplines, from neurologists and GPs to physiotherapists, speech therapists, occupational therapists. All this eases pressure on families and carers like Mildred and many others.
Malta also gives access to most PD medications through the government free at the point of use. The same can be said when it comes to any required surgery. This is available ‘without the need to travel,’ Clark specifies, ‘and this is also free, which I will point out is not the case for all European countries.’
An important role the MPDA has is its dissemination of information on how to access support services which may be required outside the family network. The Active Ageing community, Clark tells us, provides services like a carer at home, meals on wheels, home help, and many more. ‘Some aids are free and some are subsidised,’ Clark explains. ‘It is so important that people know they are not alone.’
Dancing to better health
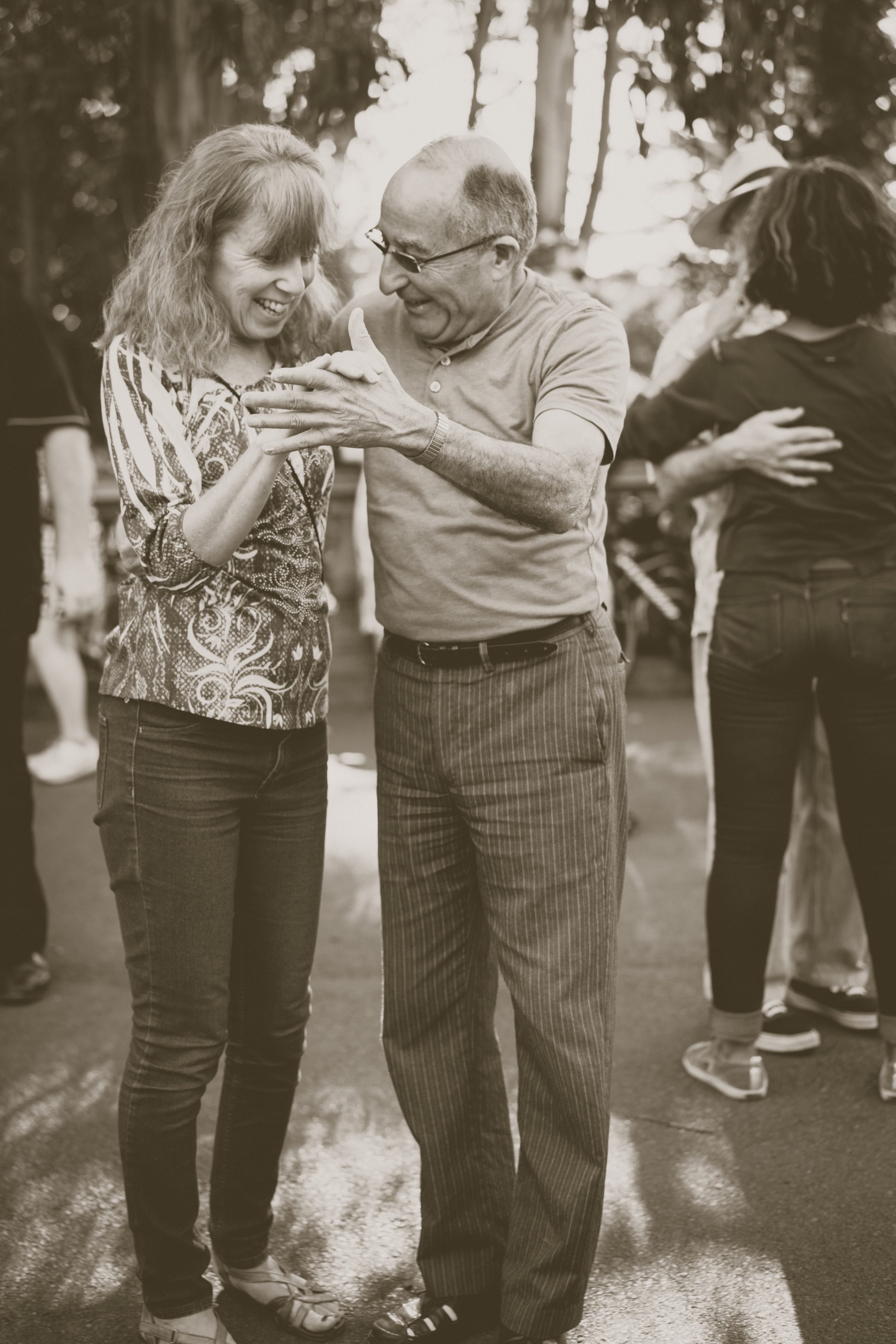
Mildred has nothing but wonderful things to say about a special group the MPDA introduced her to — Step Up for Parkinson’s (SUFP).
SUFP are not only dance classes for people with PD and their carers, but a community of people dedicated to uplifting one another.
Dancer Natalie Muschamp founded the organisation around 2016 and hasn’t looked back since.The binding philosophy is to help maintain physical activity of motor movement through dance, all while allowing the person with PD and their carer to bond and enjoy doing something together that isn’t about service.
‘When you have a disease or become a carer, you can lose your identity,’ Muschamp explains. ‘When [our participants] come to the class, they’re just two people and not a sick person and someone taking care of them. We sometimes even separate the couples. We put a lot of emphasis on this. And we encourage them to live their own lives. Some people, even after losing their partners, they continue to come. They regain some of their agency here.’
‘When you have a disease or become a carer, you can lose your identity,’ Muschamp explains. ‘When [our participants] come to the class, they’re just two people and not a sick person and someone taking care of them.
Of course, there is always room for improvement.
A concern Clark, Mildred, and Muschamp all have is that there are no specialised services tailored specifically for PD — neurologists, PD nurses, therapists, etc.
‘The lack of PD awareness people have at first hand’ is another point Mildred brings up. ‘There are so many misconceptions surrounding the condition,’ she said, ‘which often lead to added difficulties for people with Parkinson’s. To give a few examples, non-motor symptoms, such as hallucinations and impulsivity may easily lead to conflicts within the family unless they are recognised and understood. Slowness and rigidity may force people with Parkinson’s to take longer to cross the road or pay at the counter, leading to undeserved frowns or the tendency of rushing them, often quite unkindly.’
The fact that so many people don’t know what it is like to live with PD creates isolation and damaged relationships across the board. ‘The system needs to address not only the physical part of PD but also the mental, emotional, and social burdens it carries,’ Mildred encourages.
And while both MPDA and SUFP are doing their best to keep making positive changes, there is no escaping the biggest hurdle of all.
‘Co-ordinating regular and timely sessions between health professionals (from both the private and public sector) for people with PD is quite a challenge, due to reduced resources,’ explains Clark. ‘This means leaving people waiting longer or not receiving the regularity of sessions they need to manage their condition.’
The COVID effect
SUFP are also struggling with funding, especially as classes cannot happen in the real world anymore. ‘A lot of our participants struggle with the online thing,’ she explains, ‘and it’s worrying.’
‘For us not going to the gym, it will have an effect on our jean size. But for people suffering with Parkinson’s, it’s much more than that. Some of our participants started declining,’ she reveals sadly.
Ever adapting and creative, Muschamp tried to go around this by repurposing the footage from a cancelled tour with SUFP participants performing in shows all around Malta into a feature length documentary called One Day We Will Dance Again and a TV show called Step Up.
The show will air on ONE TV from January through to June of 2021, providing 15 minutes of daily exercises for the elderly and people with disabilities. ‘Amy, Mildred, Michelle, Roberta, Rowanne, myself, and everyone else — we’re currently in the middle of filming at the moment. Now we just need a good handful of sponsors to come forward — we have adverts to sell!’ she laughs, slapping the table, determined as always.
Knowing full well how infectious her energy is, Muschamp explains where it stems from — community. ‘These people are my people. My family,’ she says. ‘I can’t stop.’
The same goes for Clark. ‘When we see a smile on everyone’s face every month during our [MPDA] meetings, we know that the work we do is meaningful, and this really pushes us to continue to do what we do well,’ she says.
‘It is crucial not to live with PD alone,’ Mildred says, ‘be it the diagnosed person or the one accompanying them, whatever the stage of PD. Get in touch with the MPDA. The committee will be happy to assist them and direct them to any professional healthcare that they may require. And go to the dance classes when they start again. It makes a difference.’
‘We have to remember the bigger picture,’ Muschamp asserts. ‘What if the carer disappears? What if something bad happens to them? What then? The person with PD would need to be institutionalised sooner. The state would need to put even more resources into their care, and the result would be nowhere near as effective, because family is always family. And that does not serve our community. Caring for the carers. That serves our community.’
Artificial Intelligence (AI) is revolutionising the world. We have self-driving cars, algorithms determining future market patterns, and computers diagnosing disease. We believe that AI is supporting huge developments in healthcare.
‘Man-flu’ memes and the celebration of women’s endurance hide the reality that the medical world routinely downplays women’s pain and disease. Miriam Calleja takes a closer look.
We often hear that women are more tolerant to pain than men. Many are also proud of it. However, in the famous game-changing paper titled ‘The Girl Who Cried Pain: A Bias Against Women In The Treatment Of Pain’ the authors Diane E. Hoffman and Anita J. Tarzian found that contrary to popular belief, women report more severe levels of pain, more frequent pain, and pain that lasts longer than men’s. Three Maltese women found out the hard way that confiding in medical practitioners does not always lead to help.
Culture and gender frame our behaviour around pain perception. Boys were, and some still are, told not to express pain by crying or showing emotion. Girls were told to calm down and not make a fuss. Pain meant weakness. Our language lacks the vocabulary to adequately describe pain. In ‘On Being Ill’, Virginia Woolf writes: ‘English which can express the thoughts of Hamlet and the tragedy of Lear, has no words for the shiver and the headache… The merest schoolgirl, when she falls in love, has Shakespeare and Keats to speak for her; but let the sufferer try to describe a pain in his head to a doctor and language at once runs dry.’
Gendering pain
By analysing a number of studies, Hoffman and Tarzian found that women are ‘more likely to be treated less aggressively in their initial encounters with the healthcare system until they prove that they are as sick as male patients.’ This is a phenomenon known as the Yentl Syndrome. In other words, doctors may brush female pain off as fabricated or exaggerated. This can impact diagnosis, disease progression, and treatment plans —delaying care and fueling mistrust.
Prescribing uterus removal when a woman was ‘rebellious’ may seem like ancient history, but that bias has not fully retreated. Until the early 1990s, women were mostly excluded from clinical research studies and trials in medicine. What we knew about the body, about disease, and about medicine was based on men. Drugs that didn’t work on men, but might have worked on women, were discarded. With incomplete data, the medical world may have lost opportunities to improve women’s health. Have today’s healthcare professionals been trained to counter this gender bias?
Another doctor later referred Karen for an MRI, and the tumour was detected — a life or death analysis.
Antonia* doubts that. As a teenager she developed digestion problems and nausea every time she ate. When she complained, her family doctor downplayed the problem and suggested that she should just stop eating for a couple weeks. After this shocking response she ignored the issue for a long time, suffering in silence. Another doctor chalked it down to ‘growing pains’ and did not recommend a colonoscopy, even though Antonia asked for it.
Having received no satisfying response from her visits to medical professions, Antonia decided to do her own research, discovering that her symptoms matched the description of a condition called Crohn’s. Because of her constant discomfort and pain Antonia had no choice but to persist until she was granted testing and the correct treatment after years of suffering. This means that two doctors would have left her inflamed digestive system untreated, risking further damage.
Illustration by Gabriel Izzo
‘It is just a phase’
Women are often told that their ailments are due to stress or other emotional factors. A little rest would solve the problem; it is just a ‘phase’. Some doctors would call a woman insisting on referral for further testing a hypochondriac, even in the presence of positive clinical tests (see e.g. Samulowitz et al. 2018 study and numerous articles in the New York Times, The Atlantic and elsewhere). Thankfully, there are enough doctors who look beyond textbook-like symptoms. They make it a point to listen and investigate as much as necessary. Yet the burden of finding a practitioner ready to listen lies with the patient.
Karen visited her gynaecologist complaining of headaches and substantial weight gain. Test results revealed a high prolactin level, which is normally produced during pregnancy or right after giving birth. Yet when Karen asked to be referred for an MRI to investigate for tumours in the pituitary gland, the doctor refused, telling her that she was ‘making a fuss’. Another doctor later referred Karen for an MRI, and the tumour was detected — a life or death analysis.
Some doctors would call a woman insisting on referral for further testing a hypochondriac, even in the presence of positive clinical tests.
Gynaecologists feature often when discussing gender bias. Without systematic training to counter biases, women are left to ‘shop around’ for a gynae that doesn’t shame them or belittle their wishes. This is surprising for a profession specialising in women’s health.
Reproductive issues open another can of worms. Some women who decide not to have children are treated as though they don’t know what they’re doing. Their doctors imply that the patient will inevitably change their mind, or try to guilt the patient into considering the feelings of a hypothetical man they might meet.
You would think that commitment to bear biological children would be respected, but women who undergo IVF are often treated with insensitivity too. Sandra* and her husband had a harrowing story to tell me. Sandra’s gynaecologist decided to immediately hurry her to IVF after the first visit about their concerns at not being able to conceive. The gynaecologist was rarely present for her many appointments at hospital, leaving Sandra to be passed from one doctor to another, internally examined by various doctors without explanation or prior request for consent. With the exception of one doctor, none of them introduced themselves. All along she tried to ask questions, but was kept in the dark about the situation, going along with the doctors’ instructions but losing trust. The outcome of the first procedure was unsuccessful, and because of how traumatising all this felt, the couple decided not to try again.
Unlearning the bias
Pain is subjective and difficult to measure. An individual’s tolerance to pain is affected by various factors, and pain perception may change with time and experience. Pain causes distress, which makes it difficult to measure objectively. So how can overworked doctors make the best possible assessment?
In her thesis titled ‘The Chronic Pain Management Service: Awareness and Perceptions Among Healthcare Professionals’ (University of Malta, 2008), Maria Campbell studied pain perception in other healthcare professions in Malta back in 2008, finding out that outdated attitudes have not been challenged. She writes, ‘Incomplete knowledge, outdated attitudes, myths, and misconceptions about pain and its management contribute to unsafe, inadequate, and inappropriate pain management.’ Medical practitioners wanted to be more up-to-date: ‘The need for information in the form of leaflets, seminars, and continuing education was echoed in the overall answers (90%) of the close-ended question and in the statements declared by participants.’ But before this training becomes systemic, the radical act of listening to women is a good place to start.
* Name has been changed
Further reading:
Fassler, J. ‘How Doctors Take Women’s Pain Less Seriously’. The Atlantic. October 2015.
Hoffman D.E., Tarzian, A.J. ‘The Girl Who Cried Pain: A Bias Against Women In The Treatment Of Pain’. Journal of Law, Medicine & Ethics, Vol. 29, pp. 13-27, 2001.
Campbell, M. ‘The Chronic Pain Management Service: Awareness and Perceptions Among Healthcare Professionals.’ University of Malta. June 2008.